EMA admitted that on July 16th, 2022, there were 46,618 accumulative Deaths in Europe alone and directly correlated to experimental mRNA-containing injections
by
Robert Gorter, MD, Ph.D.
(with thanks to Frontnieuws)
July 24th, 2022
A report from Harvard Pilgrim Health Care, Inc. from 2011 for the United States Department of Health and Human Services (HHS) states that less than 1% of all adverse events after vaccines are ever reported to VAERS.
Although 25% of outpatients experience an adverse event, less than 0.3% of all adverse events and 1-13% of serious adverse events are reported to the Food and Drug Administration (FDA).
Likewise, less than 1% of vaccine unwanted side effects are reported. Low notification rates prevent or delay the identification of “problematic” drugs and vaccines that endanger public health. There is a need for new surveillance methods for the side effects of drugs and vaccines.
https://healthimpactnews.com/wp-content/uploads/sites/2/2022/07/ahrq-vaers-report-2011.pdf
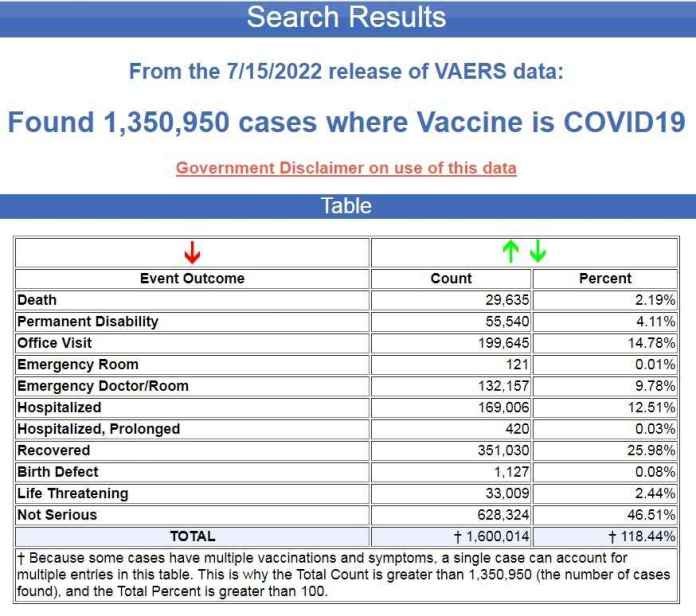
There have now been more deaths and side effects of vaccines reported to VAERS after COVID-19 vaccines in the past 20 months than in the entire previous 30 years for all FDA-approved vaccines before the emergency use authorization of the COVID-19 shots in December of 2020. (833,968 cases, 9,279 deaths – source ).
46,618 deaths and 4,682,268 injuries in EudraVigilance
The European database (EEA and non-EEA countries) of suspected drug reaction reports is EudraVigilance, audited by the European Medicines Agency (EMA), and they now report 46,618 deaths and 4,682,268 severe injuries after injections of five experimental COVID-19 injections.
Of the total number of registered injuries, almost half (2,106,816) have serious and usually life-long injuries and disabilities.
“Severity provides information about the suspected adverse effect; it can be classified as ‘serious’ if it corresponds to a medical event that results in death, is life-threatening, requires hospitalization, leads to another medically important condition, or prolongation of existing hospitalization, leads to permanent or significant disability or disability, or is a congenital/birth defect.”
A Health Impact News subscriber in Europe prepared the reports for each of the four COVID-19 recordings we include here. It is a lot of work to tabulate every response with injuries and deaths, as there is no place on the EudraVigilance system we have found where all the results are tabulated, Brian Shilhavy writes.
Here is the summary data through July 16, 2022.
Total responses for BioNTech/Pfizer mRNA vaccine Tozinameran (code BNT162b2, Comirnaty): 21,999 killed and 2,418,846 severe injuries through 07/16/2022.
Total responses for the mRNA vaccine SPIKEVAX/mRNA-1273 (CX-024414) from Moderna: 12,225 killed and 773,142 severe injuries through 07/16/2022.
Total reactions to Oxford/AstraZeneca vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19): 9,318 deaths and 1,318,927 severe injuries through 07/16/2022.
Total responses to Johnson & Johnson‘s COVID-19 vaccine JANSSEN (AD26.COV2.S): 3,076 dead and 168,267 severely injured until 07/16/2022.
Total responses to Novavax’s COVID-19 vaccine NUVAXOVID (NVX-COV2373): 0 deaths and 3,086 severe injuries through 07/16/2022.

4,358 dead babies in VAERS after COVID-19 vaccines
The latest update in VAERS shows 4,358 fetal deaths after COVID-19 vaccines were injected into pregnant women and women of childbearing age.
| Table |
| Vaccine/Manufacturer | Count | Percent |
| TOTAL | † 4,649 | † 106.68% |
| COVID19 / PFIZER/ BIOTECH | 3,396 | 77.93% |
| COVID19 / MODERNA | 1,058 | 24.28% |
| COVID19 / JANSSEN | 151 | 3.46% |
| UNK / UNKNOWN MANUFACTURER | 22 | 0.5% |
| COVID19 / UNKNOWN MANUFACTURER | 16 | 0.37% |
| HEPA / UNKNOWN MANUFACTURER | 2 | 0.05% |
| TDAP / GLAXOSMITHKLINE BIOLOGICALS | 1 | 0.02% |
| TD / SANOFI PASTEUR | 1 | 0.02% |
| IPV / SANOFI PASTEUR | 1 | 0.02% |
| FLUC4 / SEQIRUS, INC. | 1 | 0.02% |
| † Because some cases have multiple vaccinations and symptoms, a single case can account for multiple entries in this table. This is why the Total Count is greater than 4,358 (the number of cases found), and the Total Percent is greater than 100. | ||
(Source: National Vaccine Information Center / VAERS Database Fetal deaths July 2022_files/style.css).
This has got to be the saddest, criminal activity of Big Pharma and the FDA, allowing these COVID-19 injections to be injected into pregnant and young women.
Pfizer had data showing how dangerous these injections were for pregnant women, but the FDA approved it anyway.
The United States Food and Drug Administration (US-FDA) had asked 75 years to release the documents they viewed from Pfizer before granting emergency use approval for the Pfizer-BioNTech BNT162b mRNA “vaccine” (Comirnaty) against SARS-CoV-2, which can cause COVID-19.
However, a judge overruled this and issued a court order that the documents be released in large monthly installments. An absolutely shocking array of data was brought to researchers’ attention: They are not new. They come from a document that was part of the data dump that was already released in May 2022. However, we want to help my fellow scientists to ensure that this science is widely distributed around the world.
We have long advocated that our children be kept out of the mass conflict over the science behind COVID-19. In our opinion, adults can make their own risk-benefit analysis as to whether they want to receive any of the current COVID-19 vaccinations. But far too many adults make these decisions based on pseudoscience or even propaganda, data from flawed studies, misinformation, and outright misinformation disseminated by physicians and public health officials, many of whom are not qualified to speak out on anything in the world. the field of vaccinology. We have never felt comfortable using these injections in “children, adolescents and young adults of childbearing potential.“
The highest quality data for the evaluation of a new drug comes from clinical studies. That’s because these kinds of experiments in humans are usually well-controlled and involve what’s called “active monitoring”; there is a follow-up to assess safety and efficacy. Therefore, the clinical testing phases should never be compromised. With this in mind, let us take a look at a stunning array of data that Pfizer provided to the US FDA.
The data in this document was collected up to February 28, 2021. Notably, on page 9 the safety concern based on the US Pharmacovigilance Plan includes “missing information” on “Pregnancy and Breastfeeding Use”. The data collected up to the end of February 2021 were of too small a sample size (ie # pregnant or lactating women) to justify use in these populations. However, here are the data available at the time on outcomes in pregnant women who received Pfizer’s COVID-19 vaccine; this is quoted from the top part of table 6 (I have italicized and/or bolded key points)…
Pregnancy cases: 274 cases, including:
– 270 cases in the mother and 4 cases in the fetus/baby, representing 270 unique pregnancies (the 4 cases in the fetus/infant were linked to 3 cases in the mother; 1 case in the mother involved twins).
– The pregnancy outcomes for the 270 pregnancies were reported as spontaneous abortion (23), outcome pending (5), preterm birth with neonatal death, spontaneous abortion with intrauterine death (each 2), spontaneous abortion with neonatal death, and normal outcome (each 1). No outcome was given for 238 pregnancies (note that for each twin, 2 different outcomes were reported, and both were counted).
Apparently, the results will never be known for 88% (238/270) of pregnancies. Why was the follow-up of these cases so abysmal?
NutriTruth has a nice chart on their website that summarizes the results of cases where follow-up data was available:
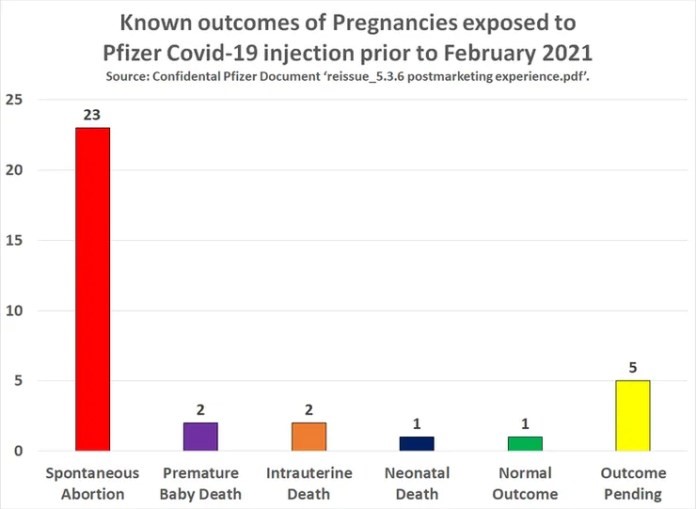
It appears that data would be available for five of the pregnancies, but these outcomes were unknown at the time of the writing of Pfizer’s paper. So there are solid data available from 29 pregnancies. One out of 29 of these pregnancies had a “normal” outcome. That means 28 of the 29 babies have died! That’s a death rate of 97%. It is of little importance at this point what reliable data set you look at to determine a “background” death rate, none come close to 97%. Spontaneous abortions are more common than many people think, but, again, they are nowhere near the rate in this study. Even in the case of the “normal outcome” it means there was an apparently healthy baby.
We looked at Pfizer’s preclinical data on reproductive toxicity, and it’s fatally flawed. One of the problems was “vaccinating” only the females; apparently, people had forgotten that “it takes two to tango”. Also, the rodent models were used to express the low-affinity version of the receptor for the spike protein encoded by the “vaccines”. Humans express the receptor with high affinity. This means that the rodent models are unable to reveal the toxicity that could be associated with the spike protein. In short, the preclinical studies could not provide any assurance that Pfizer’s vaccine would be safe in the context of pregnancy.
Our group has been working with scientists and doctors on the “real-world” studies after the launch of the vaccine on pregnancy and the COVID-19 injections. They are all very flawed. Real-world studies should never have been approved on the basis of the data presented by Pfizer.
Many countries have forced Pfizer’s COVID-19 “vaccine” on pregnant women, often through mandates. This was done with the full blessing of their obstetrics and gynecology associations. With this data in hand, will the obstetricians and gynecologists continue to make these recommendations? Ultimately, couples who are experiencing or wishing to experience a pregnancy must take responsibility for informing themselves in order to enable fully informed consent. Too many obstetricians and gynecologists are either too superficially trained in the immunological subdiscipline of vaccinology, or they are too afraid to contradict a narrative that punishes deviant behavior. Some doctors are starting to speak out about this. Unfortunately, their one-off personal observations are simply considered anecdotal. As a scientist, however, we have been trained to observe the cumulative nature of these reports; not to dismiss them outright, and to use them to formulate legitimate scientific questions.
If you or your baby have experienced any problems after the vaccination, please tell your doctor. They are obliged to report an undesirable effect, without expressing an opinion on whether they think there is a connection or not. The accumulation of these reports is the only way scientists can help detect safety signals during a public rollout of a new medical product.
A 97% death rate in babies born to pregnant mothers who were “vaccinated” is staggering. And this came from Pfizer’s own clinical trial data. This points to a massive failure in the public health regulatory process. The public, which public health regulators should serve, should demand accountability from these government-run institutions.
If we were a regulatory scientist reviewing Pfizer’s pregnancy outcomes, we would in no way have ever supported the use of their inoculation in pregnant women. And we would never have allowed “real-world” data from flawed studies to take the place of sound preclinical and clinical trials. Nor would we be silent about this knowledge. Regulators who know better should start raising their voices.