Dutch and EU corona policy causes more suffering and death than it wants to prevent

A corona army parade
More and more clinical doctors and psychologists are writing about the devastating measures against Covid-19.
The measures against the coronavirus are perhaps more deadly than the virus itself. That is what psychologist Michaela Schippers, PhD, and the professor Dr. Robert Gorter from the USA, Germany and the Netherlands, and clinical ethicist Dr. Erwin Kompanje say, who together wrote razor-sharp articles about the effects of the corona policy. “It is precisely the people that they wanted to protect were seriously weakened by this policy.”
Dr. Robert Gorter is also very concerned about the use of retroviruses (such as HIV that causes AIDS) in producing new viruses as well as new vaccines.
Michaela Schippers, PhD, is a psychologist and professor of Behavior & Performance Management at the Rotterdam School of Management. She conducts research into goal setting, group behavior and personal happiness. Erwin Kompanje is a philosopher and clinical ethicist at the Erasmus Academic Medical Center, which has functioned as the epicenter of the Dutch corona approach in recent months. Together they wrote the article “For the Greater Good? The Devastating Ripple Effects of the Covid-19 Crisis. ”
How do clinical medical ethicists and psychologists come together for a thorough publication on the draconian measures against Covid-19 in most European countries?
We were concerned about the measures being taken. When people go into lockdown, it is fierce, even if it only lasts for two weeks. But it soon became apparent that it was going to take longer. People were terrified, vulnerable people hardly had access to care and psychological support anymore, for example my mother was locked up in the retirement home. I thought: that will have enormous negative consequences in all kinds of areas: social, psychological, economic, let alone public health. But around us there was hardly any attention for criticism. People waved it away.
A policy was put in place to achieve a goal. The original goal was: to reduce the influx of patients to care, to ensure that it did not become overloaded and that even more people would die. At first that seemed to work, the curve flattened out a bit. But every drug has side effects, even now. All doctors and who are ethically committed to patients, it is their task to continuously balance the good and bad outcomes of a drug used. “What to do if the drug is worse than the disease itself ……?
A fearful society full of paranoia is emerging
In various articles, many academics systematically explain the major adverse effects of lock downs. An economic crisis, increasing inequality, rapid increase in suicides, inhumane conditions in nursing homes, etc. They also argue that the measures endanger public health. How can that be?
We are resistant to all kinds of diseases because we have an immune system. This is usually very capable of rendering all kinds of pathogens harmless. But we know that the functioning of that immune system is influenced by food and the environment. Stress, for example, slows down your resistance, while valuable social contact, touch and sunlight boost your immune system. During the lockdown period, social contact had to be minimized or even prevented, people could not go outside and, according to various studies, and they experienced much more stress and anxiety. You could say that healthy adult people still had some room for maneuver, but the frail and the elderly did not. What really triggered me at one point were the messages coming from the nursing homes, care homes and hospices. People were placed in isolation, were no longer allowed to see their families and loved ones and could no longer sit in the garden.
We call that the “corona paradox.” That we actually weaken the people we want to protect. This is reflected on many fronts. For example, the fact that people with other medical conditions – such as cancer, heart complaints or neurological problems – have had less or even no access to care in recent months because everyone was focused on Covid-19. And it has been calculated that the global economic downturn could eventually lead to as many as 100 million deaths. The lockdown was a horse remedy. ”
And we wonder why politicians and wealthy philanthropists in particular want to push for the next lock-down …
Dr. Gorter: by the way, what is the definition of a Philanthropist?
A Philanthropist is someone who publicly gives 10% of what he has stolen privately.”
“Corona puts a magnifying glass on differences between rich and poor”
Let’s go back to March 2020. The intensive care units became full and we were left with a number of patients that were increasing exponentially. Erasmus Medical Center in Rotterdam was the epicenter of the Dutch corona fight with a press conference almost daily. Surely it was not an inconceivable scenario that patients would die in the corridors of hospitals a few weeks later? Isn’t it necessary to intervene strongly?
In the beginning it looked like something was going on. It started in Brabant, where the first patients with Covid-19 probably showed up. We only knew it from China and Italy and we had no idea what was to come. But we are an organized country, aren’t we. We soon realized in the hospital that the patients would never be in the corridors here. Not even when maximum IC capacity came into view. At that time it was already clear that in Germany, where the peak had already passed, there were still three thousand ICU beds available. ”
There was certainly something going on. At one point I even taught my son – who was still four at the time, he just turned five – to call the emergency number. I had heard about a woman in America whose child had sat next to her for two nights while she was already dead. That was an absolute horror scenario.
But very soon more knowledge about the virus was gathered and it became apparent in May 2020 that the average age of the people who died in the Netherlands was 82, for example. ” In Germany this is exactly the case: average age of people who died of Covid-19 is 82 years (University of Hamburg, Germany)
“We live in the illusion of immortality. But at some point we will die from something”
It is estimated that absolutely no more than nine thousand people have died in the Netherlands with a population of 17,5 million.
Of the 6,000 patients who died out of 17,500,000 Dutch citizens, who have been counted in the Netherlands so far, only fifteen were younger than 40. By comparison: every year 2700 people in that age category in the Netherlands die from another cause of death, for example a traffic accident, smoking or cancer. Of the 17,5 million inhabitants, approximately 46 percent are under 40. Based on fifteen deaths, there is a 0.00019 percent chance that you will die from Covid-19 in that age group. That is statistically absolutely negligible and makes these current Lock-Down measures absurd and criminal. ”
And more and more documentation proves that young people have overestimated the chance of dying from Covid-19 at least five hundred times. ”
The vast majority of the deceased are old and, moreover, there was often – in any case proven by 70 percent – there was clear comorbidity: underlying serious suffering. Covid-19 has almost only affected older people with an average age of 82 years and people with severely failing immune systems. ”
“We will increasingly be asked how much money and general social and economic suffering we have left for an extra year of life gained”
The end is approaching!
And they would otherwise have died next year?
Yes, that chance is very high. Every autumn, thousands of people die of influenza, the seasonal flu, in the care and nursing homes. As you get older, your immune system starts to function worse. That’s why old people are more prone to all kinds of ailments. Most men die around 80-85, women around 85-89. A single exception becomes 90, a very single exception 100, but then it’s done. At one point I heard someone say on the radio that his mother, who had just died of Covid-19 at the age of 84, could have turned 94 if the measures had been more stringent. While: in that period of ten years, there are still a number of major hurdles to overcome for someone of that age. We live in the illusion of immortality. But at some point we die from something. That’s handy too, because a lot of children are now being born at the front. ”
isolation nursing homes and homes for the elderly
During the epidemic, it became very clear that a certain frame had been chosen: “war” with an “unknown enemy”. There were daily updates on the number of “victims”, there was talk of health workers on the “front line”. These are all concepts and metaphors from warfare.
In the beginning there was still a little dissent, even in the mainstream media. That Covid-19 was not much more severe than an average flu wave, for example. But that soon died down. Apparently only one course had to be sailed. The editor-in-chief of de Volkskrant literally confirmed in a radio interview that some information did not end up in the newspaper: banned by “Hoger Hand” (read government). ”
The great thing about people is that the individual is willing to make sacrifices for the big picture. Only now sacrifices are being made without meaning. The problem is, people don’t want to hear that. Cognitive dissonance occurs. They think: I have gone bankrupt, that must be for the greater good. These people literally ask us whether we want to stop sending them critical articles about the measures. ”
Corona news media
We also experience this within the universities and among academics and what must be a place for critical debate and independent thinking. And where politics and lobyists with their own agendas also like to mix.
What surprises us is that intelligent people do not realize that proportionality is completely lost here. Apparently people don’t see much further than their own noses.
It is clear that a great deal of damage has been and is being caused by the media. Every day people asked us, “Do you know how many people died today?” But that did not keep you from any disease by the way. The relentless flow of information has generated a great deal of fear and unrest: on purpose?
“There has been an increase in the number of COVID-19 positive cases because much more is being tested with PCR than 6 months ago. If more people were to have their IQ tested in this way, more morons would be found! ”
The media (on purpose?) played a very bad role. In a crisis situation, there is always less room for dissenters. We like to refer to a number of classic social experiments – from Asch and Milgram and the Stanford Prison Experiment – and they show time and again that people are eager to obey. That can be explained by the way. In prehistoric times it was sometimes also fight or flight. Someone who wanted to discuss policy thoroughly could then be deadly. But that group behavior has become dysfunctional here. Look at what we have done. And it’s not over yet: it seems to get even worse now that a “Second Wave” is “proven” by testing 100 times as many people and finding 100 times more positives makes sense. It is not without reason that we demonstrated against something for the first time in our lives. Several colleagues and we have written a letter to the Prime Minister Mark Rutte. All things we had never done before. It takes an incredible amount of time and energy as we do not the next generation to grow up in a kind of police state.”
Is that really our fear?
We do not know how many Dutch people have read the new law, but the plan is to suspend all civil liberties indefinitely. ” That is to say: to abolish all Human Rights and all democratic laws and traditions! ”
In such a 1.5 meter society, we see a lot of negative consequences for the psychosocial development of young people in particular. We are social beings. ” And, there is no scientific evidence to support the one and a half meter rule.
Corona is forcing us to a new economic system
We are not conspiracy thinkers, but a conspiracy theory has regularly turned out to be true. Look, a conspiracy theory is by definition an unproven theory. And as long as it is unproven, I say: someone else has to find out. I can still explain everything without having to have a master plan behind it. But we don’t know for sure because there is indeed consistently “fake news and censorship from the same corner.”
In a different way we need to start thinking about more “solidarity”
There has been a lot of criticism that the virologists initially set the policy. Should that be different next time?
There are a number of techniques to get around groupthink. What they have in common is that you organize reflexivity and put different perspectives together. Let another team, with philosophers, economists or behavioral scientists shoot your plan. ”
In the beginning, it was logical that both GPs and politicians listen to the virologists. They should understand best how such a virus behaves. But if it soon becomes apparent that the number of hospital admissions is declining sharply, you should also look at other perspectives. At least in the mainstream media, that has happened too little or even completely. ”
Mortality directly correlated to smoking
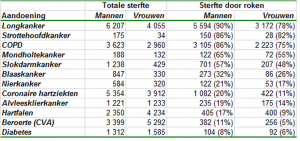
More than half of the people who smoke die from the consequences. (1-3) In the Netherlands, this is approximately 20,000 people annually (see Table 4). They die of diseases directly caused by smoking.
These figures come from the National Institute of Public Health and Environment (RIVM). It is based on a comparison of the morbidity and mortality rates between two groups: smokers and non-smokers, which further correspond on relevant characteristics (such as age, gender and level of education). This comparison shows that smokers develop certain serious illnesses much more often than non-smokers, such as (lung) cancer, cardiovascular disease, COPD and other lung diseases.
Deaths due to a number of disorders among Dutch people aged 20 and older. Reference year 2013
Percentages indicate the share of smoking in mortality in the Netherlands. Source: RIVM
The following percentage of deaths can be attributed to smoking:
85% of lung cancer deaths;
85% of laryngeal cancer deaths;
81% of deaths from COPD;
62% of oral cavity cancer deaths;
54% of deaths from esophageal cancer;
31% of bladder cancer deaths;
19% of kidney cancer deaths;
17% of pancreatic cancer deaths;
16% of deaths from coronary heart disease, including myocardial infarction;
12% of deaths from heart failure;
7% of deaths from stroke (CVA);
7% of deaths from diabetes.
On average, smokers die ten years earlier than non-smokers.
This is based on multiple large-scale international studies, in which tens of thousands of people have been followed for decades. (1-3)
Passive smoking
Second-hand smoking, or “passive smoking”, is the inhalation of tobacco smoke from the environment. According to an estimate by the RIVM, around 10,000 people in the Netherlands die annually from cardiovascular diseases as a direct result of passive smoke and several hundred as a result of passive smoke from lung cancer. An international comparative study (7) showed that the Dutch are relatively unaware of the damage that second-hand smoke can cause.
International
Globally, according to the World Health Organization (WHO), more than 7.5 million people die each year from tobacco use and 890,000 from passive smoke. (11)
There is one premature death from smoking every six seconds. (8) It is estimated that 12% of all deaths worldwide can be attributed to smoking (16% among men, 7% among women). (9)
In Europe, and certainly the Netherlands, tobacco-related mortality is even higher, because a relatively large amount of smoking has taken place here in the past. In Europe, 16% of deaths can be attributed to smoking (25% among men, 7% among women); in the Netherlands this is 21% (28% among men, 14% among women).
Diseases due to tobacco use only develop over time. At a population level, it can be seen that smoking-related death rates only rise decades after smoking has gained in popularity. The figures for the percentage of smokers and smoking-related mortality have a similar trend in most countries (see figure below). First comes an increase in smokers, first mainly men and later also women. Decades later, when smoking-related mortality rises sharply, popularity declines. However, mortality will continue to rise for years to come. (10)
Why is the government in the Netherlands and in the EU as such prepared to shut down an entire country (continent) for Corona when many times more people die, for example from (passive) smoking or alcohol consumption? Could that be because of the tobacco industry lobbying? Or does the effective lobbying of the pharmaceutical industry (BIG Pharma?) see global inoculation as the solution for all diseases on earth and that vaccination can postpone death for decades (hundreds?) of years?
We have all been in solidarity because of the Corona epidemic we think we can expect this group to change their unhealthy habits to ensure that the next pandemic is a bit milder. I am quite willing to say: lifestyle diseases are part of us as humans. But then fungi, bacteria and viruses such as the corona virus are also part of it.”
References
- Doll, R., Peto, R., Boreham, J., & Sutherland, I. (2004). Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ, 328(7455), doi:10.1136/bmj.38142.554479.AE.
- Jha, P. et al. (2013). 21st Century hazards of smoking and benefits of cessation in the United States. The New England Journal of Medicine, 368(4), 341-350.
- Sakata, R., McGale, P., Grant, E. J., Ozasa, K., Peto, R., & Darby, S. C. (2012). Impact of smoking on mortality and life expectancy in Japanese smokers: a prospective cohort study. BMJ, 345, doi: http://dx.doi.org/10.1136/bmj.e7093.
- Klijs, B., Mackenbach, J. P., & Kunst, A. E. (2011). Obesity, smoking, alcohol consumption and years lived with disability: a Sullivan life table approach. BMC Public Health, 11(378), 1-7.
- Hoeymans, N., Melse, J. M., & Schoemaker. C. . (2010). Gezondheid en determinanten. Deelrapport van de VTV 2010: van gezond naar beter. Bilthoven: RIVM.
- ITC Project (2011). ITC Netherlands Survey. Report on smokers’ awareness of the health risks of smoking and exposure to second-hand smoke. Canada: University of Waterloo.
- WHO (2013). Report on the global tobacco epidemic. Geneva: World Health Organization.
- WHO (2012). WHO Global Report. Mortality attributable to tobacco. Geneva: World Health Organization.
- Lopez, A. D., Collishaw, N. E., & Piha, T. (1994). A descriptive model of the cigarette epidemic in developed countries. Tobacco Control, 3, 242-247.
- WHO (2017). Factsheet Tobacco.